As practitioners and scientists in the field of environmental engineering, we understand that hospitals are not just healing institutions, but also complex “factories” that produce hazardous by-products. Among the various types of waste generated, liquid effluent holds a crucial position due to its ability to become a rapid and widespread vector for disease transmission if not handled with scientific precision. An effective medical liquid waste treatment system does not merely meet regulatory quality standards; it is the first line of defense in preventing environmental health crises and the spread of antimicrobial resistance (AMR).
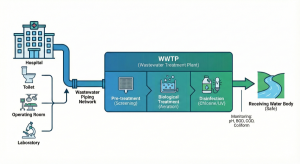
This article will deeply dissect the integrative mechanisms, from biological degradation to chemical oxidation, required to transform infectious wastewater into effluent that is safe for receiving water bodies. We at PT Mizui Osmosa Teknovasi believe that a fundamental understanding of these processes is the key for hospital sanitarians and engineers to design and operate a reliable Wastewater Treatment Plant (WWTP).
The Microscopic Threat: Why is Medical Liquid Waste Different?
Fundamentally, domestic wastewater and medical wastewater share the same basic matrix—water carrying organic matter. However, the difference between solid and liquid medical waste lies in the mobility and composition of the micropollutants within it. Medical liquid waste possesses unique characteristics that demand a much stricter engineering approach than conventional domestic waste treatment.
Pollutant Characteristics: Pathogens, Pharmaceuticals, and Chemicals
From an environmental engineering perspective, we categorize the pollutant load in hospital liquid waste into three main interacting components:
-
Biological Load (Pathogens): This is the primary differentiator. Liquid waste from isolation wards, microbiology laboratories, and operating rooms contains high concentrations of pathogenic bacteria (such as Salmonella, Shigella, Vibrio cholerae), enteric viruses (hepatitis, rotavirus), and protozoan cysts. Coliform concentrations are often thousands of times higher than in domestic waste, demanding extreme disinfection efficiency.
-
Pharmaceutical Micropollutants (Pharmaceutical Residues): Hospital effluent is a major source of pharmaceutical residues entering the environment. Antibiotics, cytotoxic drugs (chemotherapy), hormones, and analgesics excreted by patients or discarded from pharmacies are mixed in the wastewater. The presence of antibiotics in sub-lethal concentrations in the WWTP can trigger the natural selection of resistant bacteria, creating superbugs within our own biological reactors.
-
Toxic Chemical Load: The excessive use of a chlorination disinfection system on hospital floors, laboratory solvents (like xylene, formaldehyde), and heavy metals (mercury from dental amalgams, silver from radiology) adds complexity. These materials often act as inhibitors (toxins) for the decomposing bacteria in the biological treatment unit, which can cause sudden WWTP system failures.
A medical wastewater treatment system designed without simultaneously accounting for these three components will inevitably fail to meet long-term safety standards.
Fatal Consequences of Nosocomial Pollution to the Environment
If the effluent containing the dangers of medical liquid waste escapes into water bodies without adequate treatment, the impacts are catastrophic and long-lasting. We are not just talking about high BOD/COD parameters causing river deoxygenation (fish kills), but about very real public health risks.
The most serious consequence today is the spread of Antimicrobial Resistance (AMR). Suboptimal hospital WWTPs act as “breeding reactors” where pathogenic bacteria are exposed to low-dose antibiotics, develop resistance genes, and then transfer those genes to environmental bacteria in receiving rivers. This is a global threat that the WHO has dubbed one of the greatest health challenges of this century.
Furthermore, parameters like high free ammonia (NH3-N) are directly toxic to aquatic life, while phosphates from detergents trigger eutrophication (algal blooms) that destroy aquatic ecosystems. Therefore, strict monitoring of hospital waste ammonia and coliform parameters becomes a key performance indicator for the WWTP.
First Stage: Biological Process to Decompose Organic Load
In the hierarchy of the physical chemical biological WWTP process, biological treatment is often the heart of the system. Why? Because before we can effectively kill pathogens using chemicals, we must remove their “shield.” Dissolved and suspended organic matter (measured as BOD and COD) acts as a protector for pathogenic microorganisms against disinfectant agents.
Without a significant reduction in organic load, the subsequent disinfection process will be inefficient, waste chemicals, and produce carcinogenic disinfection by-products (DBPs) such as trihalomethanes (THMs).
Activated Sludge Mechanism in Reducing BOD
The most commonly adopted biological method for medium to large-scale hospitals is the Activated Sludge Process or its modifications (such as SBR or MBR).
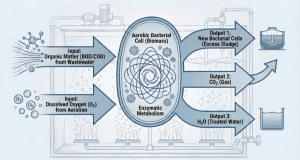
Microbiologically, the basic principle of this system is to utilize a consortium of natural microorganisms (bacteria, protozoa, rotifers) that we “breed” in an aeration tank. We provide optimal conditions for them—Dissolved Oxygen (DO) via blowers and food (organic substrates from the hospital wastewater).
Heterotrophic aerobic bacteria will metabolize carbonaceous organic matter (BOD) into new cell biomass, carbon dioxide (CO
2), and water. This process drastically reduces the biological oxygen demand in the wastewater. The key to the operational success of this system lies in a balance called the F/M Ratio (Food-to-Microorganism ratio).
-
If the F/M is too high (excess waste load), the bacteria cannot decompose perfectly, resulting in turbid effluent and poor BOD reduction.
-
If the F/M is too low (starving bacteria), the bacteria will begin to consume each other (endogenous respiration) and form sludge that is difficult to settle (pin-point floc).
As engineers at Mizui Osmosa, we emphasize the importance of controlling Mixed Liquor Suspended Solids (MLSS) in the aeration tank to keep the bacterial population optimal, usually in the range of 2500 – 4000 mg/L for conventional systems.
The Role of Aerobic and Anaerobic Bacteria in the Treatment Cycle
Although the aerobic process is dominant in reducing BOD, understanding the role of anaerobic bacteria is also crucial, especially in the context of modern medical effluent treatment technology targeting nutrient removal (Nitrogen and Phosphorus).
Hospital waste is often rich in ammonia (NH3-N) derived from urea in urine. Aerobic bacteria of the Nitrosomonas and Nitrobacter types play a role in the nitrification process, converting toxic ammonia into less toxic nitrate (NO3-N). However, nitrate is still a nutrient that can cause eutrophication.
To remove nitrate, we need anoxic conditions (no dissolved oxygen, but nitrate is present) where denitrifying bacteria will convert nitrate into harmless nitrogen gas (N2) that escapes into the atmosphere. Some advanced WWTP designs integrate anoxic zones before or after the aeration tank to achieve Total Nitrogen removal.
Anaerobic processes (with absolutely no oxygen) are rarely used as the primary treatment for hospital liquid waste due to odor risks and sensitivity to toxic chemicals, but they are sometimes used in sludge digestion or as a pre-treatment for very high-concentration organic waste from the nutrition kitchen.
Second Stage: Pathogen Elimination with Chemical & Physical Disinfection
After the effluent passes through the biological treatment and sedimentation stages, the resulting water should be clear with low BOD/COD levels (< 30 mg/L BOD). However, microbiologically, this water is still dangerous. The absolute final stage, the final barrier, is disinfection.
The goal is to achieve a specific Log Reduction Value (LRV) for indicator pathogens. For example, a 4-log reduction means eliminating 99.99% of target microorganisms. The choice of disinfection technology must consider cost-effectiveness, operational safety, and the potential for hazardous residues.
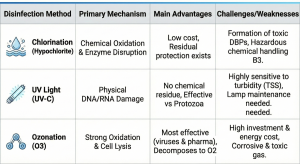
Chlorination: The Most Common Method But Requires Dose Precision
Chlorination remains the most widely used disinfection method in Indonesia due to its low cost and the availability of chemicals (usually Calcium Hypochlorite or liquid Sodium Hypochlorite).
Its mechanism of action is through the formation of hypochlorous acid (HOCl) when chlorine dissolves in water. HOCl is a strong oxidant that penetrates bacterial cell walls, disrupts enzyme metabolism, and destroys genetic material, causing pathogen inactivation.
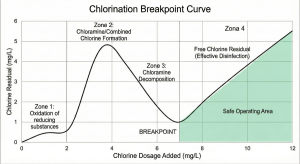
However, applying chlorination to medical waste requires a deep understanding of the Breakpoint Chlorination concept. Hospital waste contains ammonia and other organic substances that will react with chlorine first to form chloramines (combined chlorine compounds) which have weak disinfection power. Free chlorine will only effectively kill bacteria rapidly after all these interfering substances have reacted and the “breakpoint” is reached, where further chlorine addition will produce a free chlorine residual.
An incorrect dose—below the breakpoint—will not effectively kill resistant pathogens. Conversely, an overdose will result in high chlorine residues in the effluent, which is toxic to river biota and violates quality standards. General standards require a free chlorine residual of around 0.2 – 0.5 mg/L after a minimum contact time of 30 minutes in the chlorine contact tank.
Alternative Technologies: UV Light and Ozonation for Clear Effluent
Given the risk of forming toxic by-products from chlorination and the need to handle B3 chemicals, alternative technologies are increasingly favored for modern medical facilities.
-
Ultraviolet (UV) Irradiation: UV-C light (254 nm wavelength) works physically by penetrating the cell walls of microorganisms and being absorbed by their DNA/RNA. This causes genetic structure damage (thymine dimer formation), which prevents microorganisms from reproducing. UV is highly effective against bacteria and protozoa like Cryptosporidium< that are chlorine-resistant.
-
Advantages: No chemical residue, no DBP formation, extremely short contact time (seconds).
-
Disadvantages: Highly dependent on water clarity (UV transmittance). Turbid effluent resulting from biological process failure will block UV light from reaching targets, causing total disinfection failure. UV lamps also require routine cleaning and periodic replacement.
-
Ozonation (O3): Ozone is an oxidizing gas that is much stronger than chlorine. Ozone works by directly attacking bacterial cell walls (cell lysis) and oxidizing organic pollutants, including pharmaceutical residues that are difficult to break down.
-
Advantages: Highly effective at killing viruses and bacteria, capable of breaking down micropollutants and color. Ozone decomposes back into oxygen, leaving no residue.
-
Disadvantages: High investment (ozone generator) and energy costs. Ozone is a toxic and corrosive gas, requiring strict safety handling in the machine room.
As a brief comparison between methods: (Author’s Note: The original text transitions here without providing the table, leading directly into the next section).
System Integration: From Laboratory Theory to Field Installation
Designing a system on paper is different from operating it in the field. The operational reality of a hospital presents dynamic challenges that are often not accommodated in standard textbook designs.
The Challenge of Flow Fluctuation in Real Hospitals
The biggest hydraulic challenge in B3 liquid waste management at a hospital is extreme flow fluctuation. Hospitals have peak water usage hours (mornings during patient bathing, laundry activities, and surgeries) where the wastewater flow can be 3-4 times the average flow. Conversely, at night, the flow can be very low.
If this peak flow enters the aeration tank (biological process) directly, the biomass will be “shocked” (shock loading) and can be washed out to the sedimentation tank before it has time to treat the waste. This results in process failure and poor effluent.
The absolute engineering solution to this problem is an Equalization Tank. This unit acts as a buffer to accommodate flow surges and level out the organic load and wastewater characteristics (such as pH fluctuations). From the equalization tank, wastewater is pumped at a constant flow rate to the biological treatment unit over 24 hours. Without an equalization tank designed with adequate volume (usually 6-8 hours of average hydraulic retention time), the stability of the biological treatment system is nearly impossible to achieve.
Why is PT Mizui Osmosa the Right Partner for System Implementation?
Understanding microbiology theory and water chemistry is only the first step. Translating it into physical infrastructure that is reliable, durable, and easy for hospital operators to use requires specific engineering expertise.
At PT Mizui Osmosa Teknovasi, we do not just sell products; we provide data-driven engineering solutions. Our approach begins with the specific characterization of your hospital’s waste—because Type A hospital waste differs from Type C hospital waste. We integrate robust biological technologies (like MBR or Extended Aeration) with precise disinfection systems, ensuring compliance with MoEF Regulation No. P.68/2016 concerning Domestic Wastewater Quality Standards (which is often applied to hospitals) or specific regional regulations.
We understand that sanitarians need a “quiet” system—one that works in the background without constant issues. With experience in design, construction, and operational assistance for medical WWTPs, we ensure your investment protects the environment and the reputation of your healthcare institution.
For further technical discussion regarding upgrading an existing system or designing a new WWTP,
contact our engineering team for an in-depth consultation.
Academic and Regulatory References: